
Long COVID (LC) is a chronic condition that occurs after an infection with SARS-CoV-2 and is present for at least three months. LC includes a wide range of symptoms or conditions that may improve, worsen or be ongoing. These symptoms can impact individuals in all age groups and with all health statuses, often resulting in a range of physical, psychological and social challenges that may require coordinated, multidisciplinary care.
Definition
To better address and understand the needs of patients with ongoing symptoms and long-term health consequences following SARS-CoV-2 infections (also known as Post-COVID Conditions (PCC), Post-Acute Sequelae of COVID (PASC), and Long-Haul COVID), the National Academies of Sciences, Engineering, and Medicine (NASEM) convened a panel of scientific experts that developed a formal definition of LC and recognized it as an infection-associated chronic condition. NASEM adopted this definition for LC in June 2024:
“Long COVID (LC) is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least three months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
An important feature to note: “LC can follow asymptomatic, mild, or severe SARS-CoV-2 infection. Previous infections may have been recognized or unrecognized.” NASEM’s work creating a clear definition of LC aims to improve clinical management and treatment, research, surveillance, and support services. A positive COVID-19 test is not required to diagnose LC (1).
Risk Factors
Studies evaluating risk factors for LC are ongoing. Known risk factors include older age, female, smoking, obesity, preexisting comorbidities, hospitalization and admission to the intensive care unit with COVID-19 (2-4).
Prevalence
There have been significant differences in the reported prevalence of LC due to the varying definitions of LC prior to 2024 and the varying measurements and populations studied. This means that the prevalence of LC was not consistently measured.
There are three main national surveillance studies that have addressed LC: the Behavioral Risk Factor Surveillance System (BRFSS), the National Health Interview Survey (NHIS) and the Household Pulse Survey (HPS).
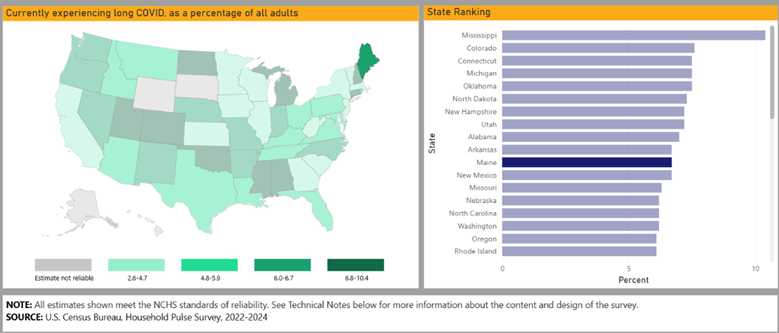
The most recent data that is available for LC prevalence in Maine is the Household Pulse Survey (2022-2024) which asked a series of questions to assess the prevalence of LC across the country. In Maine, the response to “Ever experienced long COVID”, as a percentage of all adults was 19%, “Ever experienced long COVID” as a percentage of all adults who ever had COVID was 29.5%, and “Currently experiencing long COVID” as a percentage of all adults was 6% (5).
New Interactive Long COVID Tracker
U.S. Centers for Disease Control and Prevention (U.S. CDC) has recently released new, interactive LC data visualizations that allow users to compare data compiled from the National Health Interview Survey, Behavioral Risk Factor Surveillance System, and The Tracking Post-COVID Conditions project through 2023. The visualizations provide historically published data, including:
- Prevalence of self-reported LC among U.S. adults by state and jurisdiction,
- Prevalence of LC in adults and children who have ever had and currently have LC,
- Incidence of any new conditions or symptoms in the months following COVID-19 diagnosis.
Users can view multiple analyses and review and compare LC outcomes across multiple variables like age, race, symptom or condition duration, and state or territory of residence. Updates with more current data are expected later in 2026. Click here for access the new dashboard.
Maine CDC 2026 BRFSS
The U.S. CDC BRFSS surveillance study has not included questions about LC since 2023. However, the Maine BRFSS for 2026 has seven questions about LC. The results of this survey will help provide more current data on LC in the Maine.
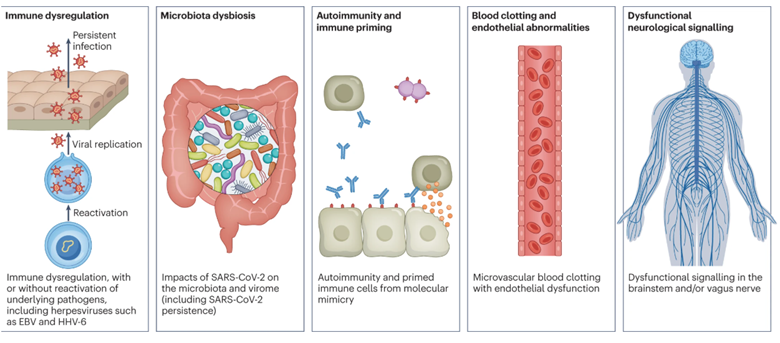
Pathogenesis
“There are several hypothesized mechanisms for long COVID pathogenesis, including immune dysregulation, microbiota disruption, autoimmunity, clotting and endothelial abnormality, and dysfunctional neurological signaling. EBV, Epstein–Barr virus; HHV-6, human herpesvirus 6; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.” Further research is ongoing (6).
Symptoms
People with LC may experience a wide variety of symptoms. Some of the most commonly reported symptoms include general fatigue, “brain fog,” sleep issues, cough, shortness of breath, cardiac abnormalities, gastrointestinal problems, and autoimmune disorders. In some patients, these symptoms subside, but for many, symptoms persist (1). Figure 3 depicts some of the common symptoms, diagnosable conditions, and the important features to consider.

Diagnosis of LC
LC is diagnosed on clinical findings. There is no specific laboratory test or standardized clinical diagnostic test. A history of a positive SARS-CoV-2 test is not required for diagnosis. A diagnosis is based on a patient’s history and physical exam findings, coupled with identifying persistent or new symptoms that arise after a COVID-19 infection, often occurring weeks or months later. As a result, clinical clarity remains challenging. It may be difficult to distinguish symptoms caused by LC from symptoms occurring for other reasons.
There have been numerous studies looking at potential biomarkers for LC. However, so far, the search for biomarkers has been elusive (7).
Diagnosable Conditions
LC is diagnosable when symptoms/conditions are intermittently or continuously present for at least 3 months. Some common conditions associated with LC are postural orthostatic tachycardia syndrome (POTS) and other forms of dysautonomia, mood disorders, cognitive impairment, migraines, chronic kidney disease, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), connective tissue and autoimmune disorders (1).
Diagnosis of LC in Children
Children may present with similar symptoms to adults. They may also present with more vague physical complaints or behavioral changes. Table 1 shows some presenting symptoms of LC by age groups. LC happens when a child continues to have symptoms for 3 months or more after having a COVID-19 infection. Sometimes symptoms change, or symptoms may reappear after feeling better (8).
Infants and Toddlers (0-2 y) | Preschool-aged children (3-5 y) | School-aged children (6-11 y) | Adolescents |
|---|---|---|---|
|
|
|
|
ICD Code
The specific Long COVID-19 code is ICD-10-CM code U09.9 (Post COVID-19 condition, unspecified).
However, it is important to note that patients with LC often have a mix of symptoms and other health conditions, tests, and treatments and are assigned other ICD codes. The clustering of co-existing conditions and potential symptoms may be valuable in informing future development of more detailed criteria for diagnosis of LC and its subtypes.
Treatment for LC
There is no specific treatment for LC. However, there are many treatments that may help manage symptoms and improve quality of life. Approved medications, physical therapy, mental health support and specialized rehabilitative therapy may be prescribed to treat specific symptoms.
The American Academy of Physical Medicine and Rehabilitation (AAPMR) published a compendium statement (2025) which emphasizes symptom-based supportive care management strategies and these important elements:
Validate the patient’s concerns and experience.
Address modifiable risk factors and comorbidities.
Focus on energy conservation strategies and carefully adjust activity recommendations to avoid post-exertional malaise (PEM).
Deliver treatment recommendations with humility as there are persistent unknowns (9).
Some experimental therapies and off-label use of medication that address persistent symptoms and conditions have also been studied. Future targeted treatment success likely relies on diagnostic biomarkers to deploy treatment and monitor effect.
Long COVID Specialty Centers
Currently, there are no specialized LC centers in Maine. Patients may be treated by their primary care clinician and/or referred to other clinicians in a particular medical specialty. LC patients may be referred out-of-state to specialized LC centers for treatment and/or involvement in new and ongoing research studies. There are several specialized LC programs in Boston, Massachusetts:
The MaineHealth specialty clinic that previously provided patients with coordinated care for ongoing COVID-19 symptoms closed in November 2022.
Impairment due to LC
While some patients with LC can continue their regular daily activities, some are not able to continue their work, school and other responsibilities due to the severity of their symptoms. An individualized assessment is necessary to determine whether a person’s LC condition or any of its symptoms substantially limits a major life activity.
People whose LC condition qualifies as a disability are entitled to the same protections from discrimination as any other person with a disability under the Americans with Disabilities Act (ADA), Section 504, and Section 1557 (10).
Prevention of LC
The best way to prevent LC is to avoid infection with SARS-CoV-2. This can be difficult since SARS-CoV-2 is circulating year round. Fortunately, COVID-19 vaccination helps protect against LC. Numerous studies show that COVID-19 vaccination prior to SARS-CoV-2 infection is associated with a lower risk of LC, demonstrating the clinical effectiveness of COVID-19 vaccination (11,12). Recent evidence suggests that the protection for those who have received COVID-19 boosters is even greater than for those who have received only the primary series (13).
Additionally, SARS-CoV-2 antiviral medication started early during acute infection has been shown to reduce symptoms in the post-acute phase. SARS-CoV-2 antivirals demonstrate protective effects for LC (14).
Ongoing Research and Learning Opportunities
Ongoing LC research aims to understand why some individuals experience prolonged symptoms after infection and gain insights from other infection-associated chronic conditions.
- Long COVID Ongoing Study in Maine at MaineHealth, Cliff Rosen, M.D. leads the Maine arm of the clinical trial, RECOVER-ENERGIZE, studying possible treatments for exercise intolerance and post-exertional malaise (PEM) related to LC. These studies will include adults who had COVID and who still have exercise intolerance or PEM symptoms.
- The RECOVER Initiative is a multi-center collaborative research arm and provides information for clinicians, researchers, and patients. The initiative supports multiple ongoing clinical trials and observational cohort studies.
- The Schmidt Initiative for Long Covid (SILC) facilitates provider education, patient care and research by hosting free public webinars, creating Communities of Practice that collaborate virtually to co-manage patient care, improving global medical infrastructure and supporting and sharing research. They support the Project Extension for Community Healthcare Outcomes (Project ECHO) institute’s LC global monthly webinar series.
- Project ECHO Global Health Initiatives offers webinars with presentations by subject matter experts, examples of emerging best practices and models of care, and a facilitated Q&A.
- Council of Medical Specialty Societies (CMSS), Long COVID Resource Repository, an updated extensive resource for primary care clinicians who face uncertainty and lack of evidence-based information to recognize, diagnose, and treat Long COVID.
Resources
Resources for Clinicians:
- National Academies of Sciences, Engineering, Medicine, Long COVID Document (PDF)
- US CDC, About Long COVID
- US CDC, Living with Long COVID
- US CDC, The Public Health Approach to Long COVID
- US CDC, Household Pulse Survey
- US CDC, Tracking Long COVID
- U.S. Centers for Disease Control and Prevention Benefits of Getting Vaccinated
- RECOVER, Pediatric Long COVID (PDF)
- Long COVID: A guide for health professionals on providing medical evidence for Social Security disability claims (PDF)
- Mayo Clinic, Long COVID: Lasting effects of COVID-19
- Yale Medicine, Long COVID (Post-COVID Conditions, PCC)
- Yale Medicine, Long COVID Articles
Resources for Patients:
- Long COVID Justice, Resource Hub
- Long COVID Families
- Longhauler Advocacy Project: to advance the understanding of Long COVID and its associated conditions and expedite solutions and assistance to Longhaulers and their families through advocacy, education, research, and support.
- Resources for people with Long COVID
References
Fineberg, H. V., Brown, L., Worku, T., & Goldowitz, I. (2024). A long COVID definition: A chronic, systemic disease state with profound consequences. National Academies Press. https://doi.org/10.17226/27768
Mandel, H., Yoo, Y. J., Allen, A. J., Abedian, S., Verzani, Z., Karlson, E. W., Kleinman, L. C., Mudumbi, P. C., Oliveira, C. R., Muszynski, J. A., Gross, R. S., Carton, T. W., Kim, C., Taylor, E., Park, H., Divers, J., Kelly, J. D., Arnold, J., Geary, C. R., Zang, C., … Moffitt, R. A. (2025). Long COVID Incidence Proportion in Adults and Children Between 2020 and 2024: An Electronic Health Record-Based Study From the RECOVER Initiative. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 80(6), 1247–1261. https://doi.org/10.1093/cid/ciaf046
Hill, E. L., Mehta, H. B., Sharma, S., Mane, K., Singh, S. K., Xie, C., Cathey, E., Loomba, J., Russell, S., Spratt, H., DeWitt, P. E., Ammar, N., Madlock-Brown, C., Brown, D., McMurry, J. A., Chute, C. G., Haendel, M. A., Moffitt, R., Pfaff, E. R., Bennett, T. D., … and the RECOVER Consortium (2023). Risk factors associated with post-acute sequelae of SARS-CoV-2: an N3C and NIH RECOVER study. BMC public health, 23(1), 2103. https://doi.org/10.1186/s12889-023-16916-w
Tsampasian, V., Elghazaly, H., Chattopadhyay, R., Debski, M., Naing, T. K. P., Garg, P., Clark, A., Ntatsaki, E., & Vassiliou, V. S. (2023). Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA internal medicine, 183(6), 566–580. https://doi.org/10.1001/jamainternmed.2023.0750
Centers for Disease Control and Prevention. (2022). Long COVID - Household Pulse Survey - COVID-19. https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm
Davis, H. E., McCorkell, L., Vogel, J. M., & Topol, E. J. (2023). Author Correction: Long COVID: major findings, mechanisms and recommendations. Nature reviews. Microbiology, 21(6), 408. https://doi.org/10.1038/s41579-023-00896-0
Gao, Y., Cai, C., Adamo, S., Biteus, E., Kamal, H., Dager, L., Miners, K. L., Llewellyn-Lacey, S., Ladell, K., Amratia, P. S., Bentley, K., Kollnberger, S., Wu, J., Akhirunnesa, M., Jones, S. A., Julin, P., Lidman, C., Stanton, R. J., Goepfert, P. A., Peluso, M. J., … Price, D. A. (2025). Identification of soluble biomarkers that associate with distinct manifestations of long COVID. Nature immunology, 26(5), 692–705. https://doi.org/10.1038/s41590-025-02135-5
Gross, R. S., Carmilani, M., & Stockwell, M. S. (2025). Long COVID in Young Children, School-Aged Children, and Teens. JAMA pediatrics, 10.1001/jamapediatrics.2025.1415. Advance online publication. https://doi.org/10.1001/jamapediatrics.2025.1415
Cheng, A. L., Herman, E., Abramoff, B., Anderson, J. R., Azola, A., Baratta, J. M., Bartels, M. N., Bhavaraju-Sanka, R., Blitshteyn, S., Fine, J. S., Fleming, T. K., Verduzco-Gutierrez, M., Herrera, J. E., Karnik, R., Kurylo, M., Longo, M. T., McCauley, M. D., Melamed, E., Miglis, M. G., Neal, J. D., … Niehaus, W. N. (2025). Multidisciplinary collaborative guidance on the assessment and treatment of patients with Long COVID: A compendium statement. PM & R : the journal of injury, function, and rehabilitation, 17(6), 684–708. https://doi.org/10.1002/pmrj.13397
Office for Civil Rights (OCR). (2021). Guidance on “Long COVID” as a Disability Under the ADA, Section 504, and Section 1557. U.S. Department of Health and Human Services. https://www.hhs.gov/civil-rights/for-providers/civil-rights-covid19/guidance-long-covid-disability/index.html
Català, M., Mercadé-Besora, N., Kolde, R., Trinh, N. T. H., Roel, E., Burn, E., Rathod-Mistry, T., Kostka, K., Man, W. Y., Delmestri, A., Nordeng, H. M. E., Uusküla, A., Duarte-Salles, T., Prieto-Alhambra, D., & Jödicke, A. M. (2024). The effectiveness of COVID-19 vaccines to prevent long COVID symptoms: staggered cohort study of data from the UK, Spain, and Estonia. The Lancet. Respiratory medicine, 12(3), 225–236. https://doi.org/10.1016/S2213-2600(23)00414-9
Watanabe, A., Iwagami, M., Yasuhara, J., Takagi, H., & Kuno, T. (2023). Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine, 41(11), 1783–1790. https://doi.org/10.1016/j.vaccine.2023.02.008
Green, R., Marjenberg, Z., Lip, G. Y. H., Banerjee, A., Wisnivesky, J., Delaney, B. C., Peluso, M. J., Wynberg, E., & Abduljawad, S. (2025). A systematic review and meta-analysis of the impact of vaccination on prevention of long COVID. Nature communications, 16(1), 10326. https://doi.org/10.1038/s41467-025-65302-0
Li, H. (2024). The efficacy of antivirals, corticosteroids, and monoclonal antibodies as acute COVID-19 treatments in reducing the incidence of long COVID. Clinical Microbiology and Infection, 30(12). https://doi.org/ 10.1016/j.cmi.2024.07.016
| Acronyms | |
|---|---|
AAPMR | American Academy of Physical Medicine and Rehabilitation |
ADA | Americans with Disabilities Act |
BRFSS | Behavioral Risk Factor Surveillance System |
CDC | Centers for Disease Control and Prevention |
CMMS | Council of Medical Specialty Societies |
COVID | Coronavirus disease |
ECHO | Extension for Community Healthcare Outcomes |
HPS | Household Pulse Survey |
ICD-10-CM | International Classification of Diseases, Tenth Revision, Clinical Modification |
LC | Long COVID |
ME/CFS | Myalgic encephalomyelitis/chronic fatigue syndrome |
NASEM | National Academies of Sciences, Engineering, and Medicine |
NHIS | National Health Interview Survey |
PASC | Post-Acute Sequelae of COVID |
PCC | Post-COVID Conditions |
PEM | Post-exertional malaise |
POTS | Postural orthostatic tachycardia syndrome |
RECOVER | Researching COVID to Enhance Recovery |
SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
SILC | Schmidt Initiative for Long Covid |
U.S. CDC | United States Centers for Disease Control and Prevention |